Are there objective measures to distinguish Speech-Language Pathologists' skill levels in providing orofacial tactile cues?
Providing tactile cues to oro-facial structures (such as lips, jaw, tongue) as part of speech therapy is not new. However, a speech-language pathologist (S-LP)
must learn new and specific hand movements and finger placements to effectively provide relevant tactile cues. Figure 1 shows speech-language
pathologist finger placement and orientation for tactile-kinesthetic-proprioceptive inputs related to vowel /u/. How might one objectively assess an S-LP's
ability to learn and provide accurate tactile cues? We discuss the innovative use of the state-of-the-art Electromagnetic Articulograph (EMA) technology to
collect objective data on S-LP skill level differences in providing tactile cues.
The study consisted of three S-LPs with different experience levels and one female adult participant who served as a model. S-LPs delivered tactile inputs to the model participant’s speech articulators, while kinematic data of mouth and finger movements were collected using an Articulograph system (AG501; Figure 2, 3, and 4). Variability of the S-LP’s finger-hand movement trajectories in 3-D space (Generalised Orthogonal Procrustes Analysis) during delivery of these tactile inputs and the consistency (cyclic Spatio-Temporal Index) of the resulting lip displacements were extracted from these data (Figure 5).
Kinematic consistency measures indicated that more experienced clinicians had lower intrinsic variability for their finger-hand movement trajectories (bottom panel - Figure. 5) and delivered tactile inputs with greater consistency (top panel- Figure. 5) relative to the clinician with less experience. Overall, experienced clinicians are more likely to recognize a client’s motor skill level and be adept at consistent and reliable delivery of tactile inputs. This may, in turn, facilitate appropriate adjustments of necessary degrees of freedom to produce articulator interactions and intelligible speech.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6330827/
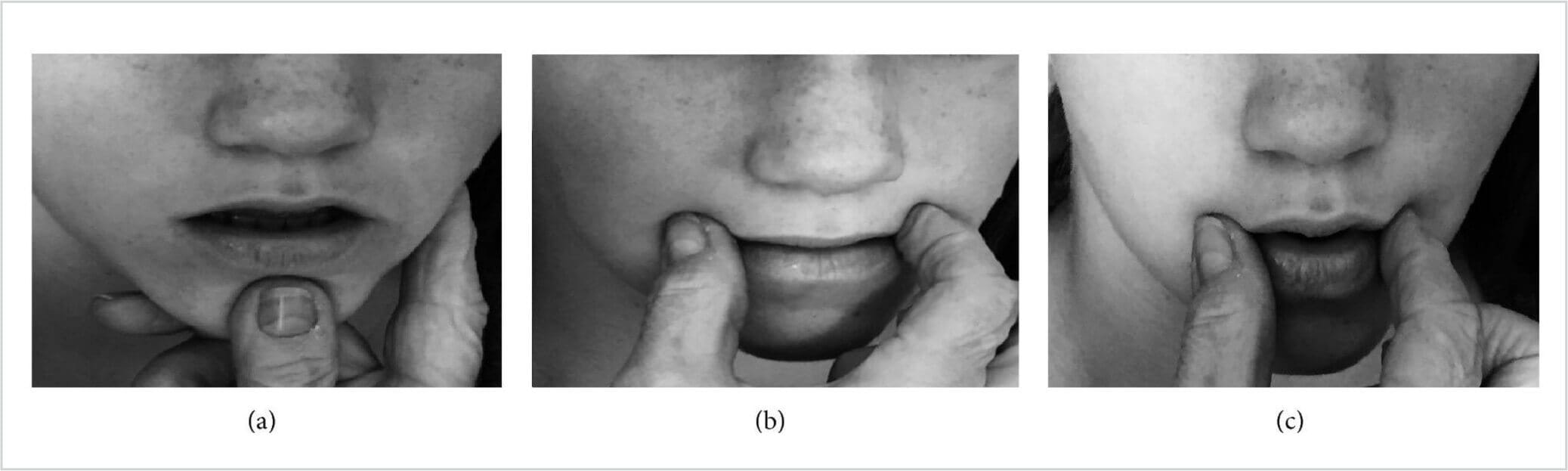
Figure 1.

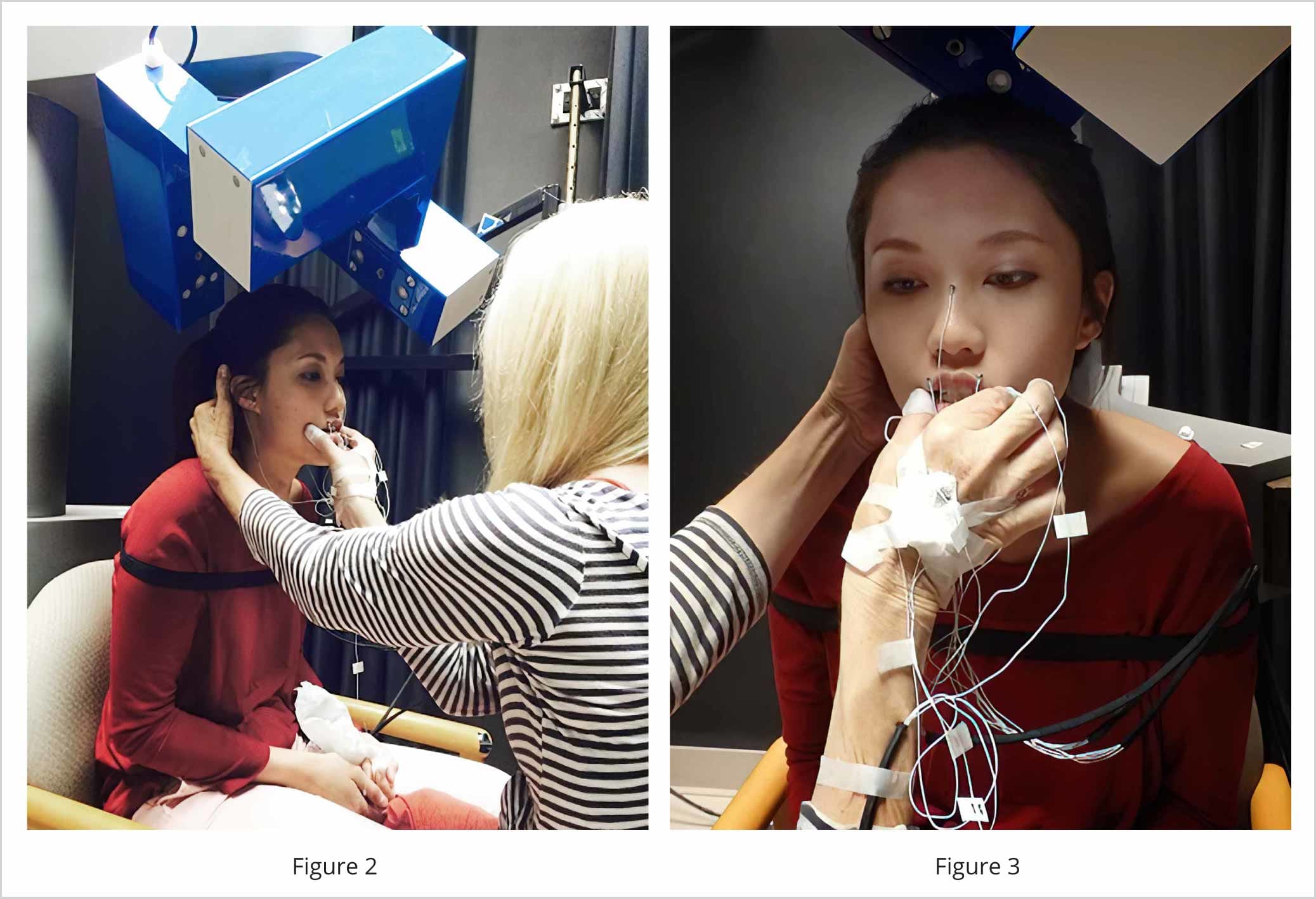
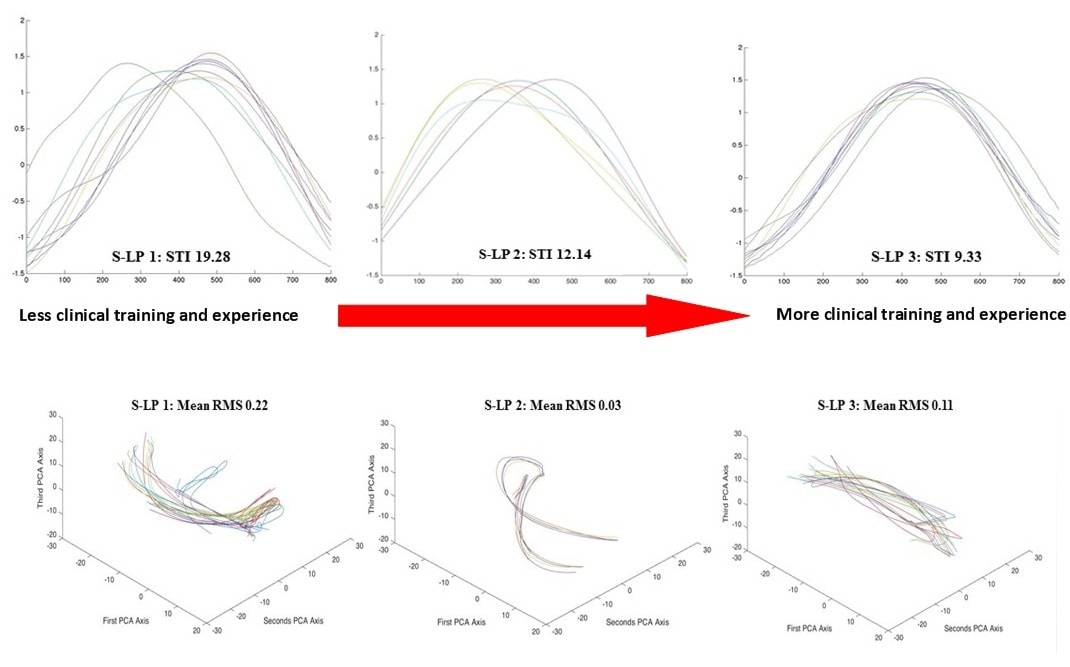 Figure 4.
Figure 4.
Figure 1. Speech–language pathologist finger placement and orientation for tactile-kinesthetic-proprioceptive inputs related to vowel /u/.
Figure 2. Speech-language pathologist providing tactile-kinesthetic-proprioceptive input to a test participant in the Electromagnetic Articulograph system (EMA AG501; Carstens Medizinelektronik GmbH, Germany).
Figure 3. Movement tracking sensors on the hand of a Speech-language pathologist in the Electromagnetic Articulograph (EMA AG501) system.
Figure 4. Kinematic consistency of upper lip movements of the participant (cyclic Spatio-Temporal Index measure; top panel) and consistency in the shape of 3-D thumb finger movement trajectories of the Speech-Language Pathologist (using Generalised Orthogonal Procrustes Analysis; bottom panel) vary as a function of clinician skill level and experience.
Reference:
Namasivayam A, K., Bali, R., Ward, R., Tieu, K.D., Yan, T., Hayden, D., & Van Lieshout, P.H.H.M. (2018). Measuring and Training Speech-Language Pathologists’ Orofacial Cueing: A Pilot Demonstration. Journal of Healthcare Engineering. https://doi.org/10.1155/2018/4323046